
Content
- 1 What is Premature Placental Abruption
- 2 Types of premature placental abruption
- 3 Causes of premature detachment of a normally located placenta
- 4 Symptoms of premature detachment of a normally located placenta
- 5 Diagnostics of the premature detachment of the normally located placenta
- 6 Treatment of premature abruption of a normally located placenta
- 7 Possible complications of premature detachment of a normally located placenta
- 8 Prevention of premature detachment of a normally located placenta
- 9 Conclusion
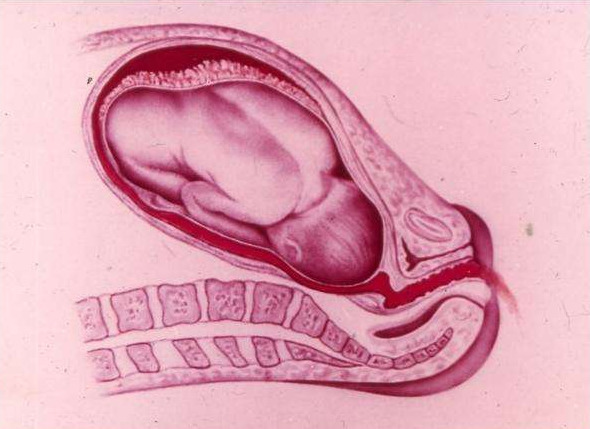
Among the many possible pathologies for the development of pregnancy, a special place is occupied by premature detachment of a normally located placenta. It is its partial or complete rejection from the wall of the uterus, which usually occurs for a period of 20 weeks or more. According to ICD-10, premature detachment of a normally located placenta has several codes, depending on the accompanying phenomena. The general labeling of a pathology that poses a threat to a woman and a child is O45.
What is Premature Placental Abruption
The etiology of premature detachment of a normally located placenta is a serious disorder that poses a threat to both the life of the mother and the life of the child. Pathology requires compulsory medical intervention. Moreover, such a phenomenon can develop not only during pregnancy, but also directly during delivery.
Attention! Risk factors for premature detachment of a normally located placenta are in the order of 0.4-1.4% of all pregnancies.
Types of premature placental abruption
There is a certain classification of premature detachment of a normally located placenta according to the type of bleeding. In addition, the PNRP can be:
- total;
- partial.
The first option is the most dangerous, since it entails a complete cessation of gas exchange between the organs of the child and the mother. It is accompanied by the inevitable death of the fetus. Partial detachment occurs in a certain limited area, it can be of the following types:
- Non-progressive. The vessels of the uterus are thrombosed, respectively, the progress of the pathological process does not occur, the threat to the fetus ceases. The course of pregnancy and subsequent childbirth is not disturbed.
- Progressive. There is a gradual increase in hematoma, and placental abruption continues. This causes a pathological course of pregnancy or childbirth.
Premature placental abruption during childbirth or during the period of gestation is also classified according to the type of localization:
- regional - often accompanied by blood flow from the genital tract;
- central - external bleeding is often absent.
With central PONRP, blood often permeates the cavity of the myometrium, which leads to damage to the muscular apparatus of the uterus
The clinical classification of premature detachment of a normally located placenta, which requires mandatory medical advice, is as follows:
- Mild degree. It accounts for approximately 40% of all cases. Characterized by blood loss of no more than 100 ml, slightly increased tone of the uterus, fetal heart rate is within normal limits. In this case, the condition of the pregnant woman is assessed as satisfactory, and the coagulation indices remain within the reference values.
- Medium degree. It accounts for about 45% of all cases, an increased tone of the uterus and pain on palpation are characteristic, the total blood loss from the genital tract can be up to 500 ml. The fetus has cardiac arrhythmias, and a pregnant woman has similar symptoms. Possible changes in blood clotting indicators for the worse.
- Severe degree. It occurs in 15% of cases, the uterus is characterized by a sharp tone, there is pain on palpation. Fetal death occurs on an antenatal basis, the pregnant woman receives hemorrhagic shock, and DIC syndrome develops additionally.
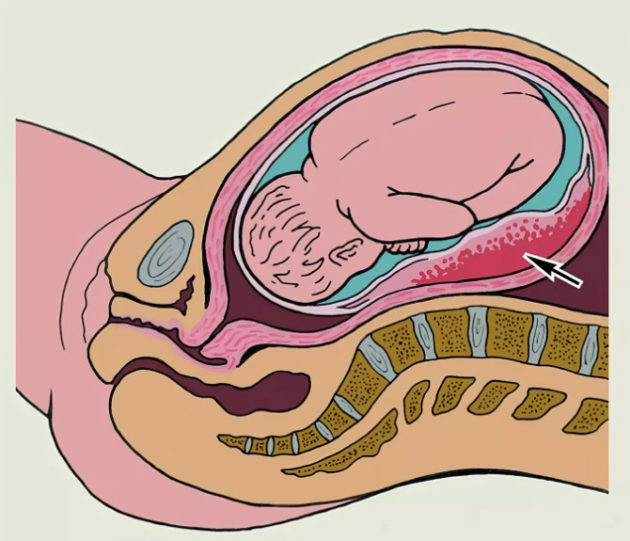
Bleeding characteristic of PONRP undergoes an additional classification:
- external - with detachment of the edge of the placenta;
- hidden - blood accumulates between the placenta and the wall of the uterus, does not leave through the genital tract;
- mixed - part of the blood flows out, the rest remains in the retroplacental position.
A warning! In severe cases, blood enters the amniotic fluid. This situation with premature placental abruption requires emergency assistance.
Causes of premature detachment of a normally located placenta
The main cause of premature detachment of a normally located placenta is the development of vasculopathy. At their core, these are vascular changes that disrupt the uteroplacental circulation. The latter arise against the background of toxicosis, somatic diseases, etc. Vasculopathy is accompanied by capillary fragility, fragility, thrombosis and multiple heart attacks.
Additional reasons for the development of PNRP:
- any inflammatory processes in the uterus;
- endometritis;
- uterine fibroids;
- post-term pregnancy;
- anatomical abnormalities.
Additionally, the following risk factors can be considered, which also contribute to the development of premature placental abruption in its normal location, - multiple births, abdominal trauma, polyhydramnios, short umbilical cord, large pure abortions, multiple births, pre-opening of the bladder, autoimmune diseases and the presence of bad habits.

Sometimes PONRP occurs as a reaction to certain drugs or blood transfusions
Symptoms of premature detachment of a normally located placenta
The main symptoms of premature placental abruption are:
- bleeding from the genital tract with the release of scarlet or dark blood;
- pain and tension in the uterus, discomfort is usually mild, radiates to the hip or lower back;
- fetal hypoxia, violation of its heart rhythm.
A characteristic sign of a severe form of premature detachment of a normally located placenta is a sharp bursting pain. It is joined by the weakness and dizziness of the pregnant woman, arising against the background of internal or external bleeding. In addition, there is a sharp tension of the uterus with its noticeable asymmetry, it is not possible to determine the fetal heart rate by auscultation.
Attention! In some cases, PONRP is characterized by the fainting state of a pregnant woman.
Progressive placental abruption is always accompanied by fetal hypoxia
Diagnostics of the premature detachment of the normally located placenta
First aid for premature placental abruption provides for the correct diagnosis of the pathological condition. If there is a detailed symptomatic picture, it will not be difficult to identify progressive PONRP by characteristic signs. It is important to take into account the presence of bleeding, hemodynamic disturbances, and fetal hypoxia.
In addition to being examined by a gynecologist, the following types of research are used as diagnostics:
- Ultrasound. Helps to establish the localization of the pathological site and its scale.
- Doppler. Allows you to identify violations of hemodynamics at the transplacental level.
- CT scan of the fetus. Allows you to identify the degree of hypoxia.
Additionally, blood and urine tests of a pregnant woman are taken, which will allow you to get a general idea of her condition.
Treatment of premature abruption of a normally located placenta
The choice of treatment tactics for PONRP directly depends on the following factors:
- the period of pregnancy when the pathology developed;
- the state of the expectant mother;
- fetal condition;
- the presence and severity of bleeding.
Pregnant women with suspected placental abruption are subject to compulsory hospitalization, regardless of the type and progress of the pathology. With a non-progressive diagnosis for up to 36 weeks, the following treatment is indicated:
- bed rest;
- a course of antispasmodics;
- the introduction of hemostatic drugs;
- therapy for anemia;
- tocolytic treatment.
Treatment is necessarily accompanied by a control ultrasound scan, a coagulogram study and Doppler ultrasound. If the detachment is progressive, the decision is made in favor of early delivery. When the birth canal is ready, the natural course of the process is possible.
If there is a moderate or severe degree of PONRP, a cesarean section is performed, natural childbirth in this case is unacceptable. KS will be shown regardless of the gestational age and the child's viability.
After removing the fetus, the state of the uterus is assessed, as well as the thickness of the myometrium. With pronounced changes, a procedure such as a hysterectomy is indicated.
Additional measures that are carried out regardless of the method of delivery:
- restoration of blood on condition of its loss;
- anti-shock therapy;
- stopping anemic processes;
- restoration of blood clotting.
In addition, the prescription of drugs of the uterotonic series is practiced.
Possible complications of premature detachment of a normally located placenta
Among the possible complications of the pathological process of PONRP, the most dangerous are:
- A high risk of blood loss in the mother, which is accompanied by hemodynamic instability, and also leads to the development of shock or disseminated intravascular coagulation.
- Transfusion from fetus to mother, additionally - alloimmunization.
- The defeat of the fetus, its death.
With chronic placental abruption, lack of water and fetal growth retardation are possible, which will further affect the developmental level of the unborn child.
Prevention of premature detachment of a normally located placenta
The main prevention of premature detachment of a normally located placenta is the mandatory and timely treatment of any pathological processes in a woman's body. It is advisable to take care of this before pregnancy.
If the diagnosis of PNRP is non-progressive and mild, the prognosis for a pregnant woman and an unborn child is very favorable. A severe form requires mandatory medical intervention, otherwise it poses a threat not only to the life of the fetus, but also to the expectant mother.

An important point is to monitor the dynamics of blood flow in the uterus and in the placenta throughout pregnancy in the presence of risk factors
A warning! Patients with established preeclampsia deserve special attention. In the absence of effectiveness during therapy, the pregnant woman must be hospitalized in the maternity hospital.
Conclusion
Premature detachment of a normally located placenta is a dangerous pathological condition that creates an increased threat to the health of the expectant mother and child. The phenomenon occurs on average in 4% of pregnant women and requires compulsory medical intervention. With the progressive form of PONRP, prompt delivery is necessary, regardless of the period of pregnancy and the viability of the fetus.
The information and materials on this site are provided for informational purposes only. You should not rely on information as a substitute for actual professional medical advice, assistance, or treatment.