
 Varicocele is a somatic disease of the genital organs in men, characterized by hypertension of veins of the lobate plexus at the site of passage of the spermatic cord.
Varicocele is a somatic disease of the genital organs in men, characterized by hypertension of veins of the lobate plexus at the site of passage of the spermatic cord.
The disease is diagnosed during puberty in adolescents, or at an older age if there are problems with spermatogenesis.
There are following traditional and progressive types of surgery to remove varicocele:
- direct exposure;
- microsurgical;
- endovascular;
- laparoscopic.
In a traditional way( with the help of direct action), cavitary operations are performed using the method of Palomo, Ivanissevich. To the progressive carry minimally invasive types of surgical intervention( the other three from the list).
Content
- Features open intervention
- progressive methods of surgical therapy
- varicocelectomy of Marmara
- Technique
- Goldstein Treatment with
- endovasal laparoscopy surgery
- Sclerotherapy spermatic veins
- Electrocoagulation
- Embolization veins
- The effectiveness of conservative and radical treatment
- Postoperative consequences
- Opinion patients
Featuresopen interventions
nissevicha is one of the first, introduced into surgical practice. However, it is considered the most traumatic.
Technique:
- is made parallel to the inguinal canal, above the entrance, a layered incision of 3-5 cm( skin, subcutaneous fat layer, fascia, sheath cord);
- secretion of venous vessels of the groinlike plexus;
- ligation, excision of dilated sites;
- layer-by-layer suturing.
Palomo surgical intervention is distinguished by a higher incision location. In the groin area,  is produced by layer-by-layer dissection. Through it penetrate into retroperitoneal tissue, directly to the testicular vein, which is ligated and crossed. The wound is sewn up.
is produced by layer-by-layer dissection. Through it penetrate into retroperitoneal tissue, directly to the testicular vein, which is ligated and crossed. The wound is sewn up.
This type of operation with varicocele requires a serious rehabilitation after it. During the first few hours, cold is placed on the inguinal zone in order to prevent edema, the development of bleeding. After that, a sterile dressing is applied to the seam, which requires regular replacement.
During the first few days a patient needs to use a suspensory to support the scrotum, avoid straining the muscles of the press. After 7-10 days, you need to remove the stitches. The following half a year is recommended to avoid increased physical exertion.
In the video clip, Ivanissevich's operation with a one-sided varicocele:
Progressive methods of surgical therapy
The microsurgical operation with varicocele has the advantage that trauma is reduced at times, rehabilitation is short-lived, and the occurrence of relapse is reduced to zero.
The progressive methods of operative therapy for varicocele include:
- microsurgical varicocelectomy;
- laparoscopic operation;
- is an endovascular intervention.
Each mode of intervention has its own characteristics, advantages and disadvantages.
Marmaru varicocelectomy
Subarginal microsurgical varicocelectomy according to Marmara is the most progressive technique used in varicocele.
 Its essence lies in bandaging the veins of the sub-tail zone, related to the lobar plexus.
Its essence lies in bandaging the veins of the sub-tail zone, related to the lobar plexus.
To date, it is used more often than other methods.
Surgical manipulations are performed using microsurgical instruments and a microscope in the following sequence:
- at a distance of 1 cm from the base of the penis do a dissection of the skin( up to 3 cm), through which the seed duct is separated;
- veins are excised at the site of expansion, then they are ligated;
- all layers are sequentially sewn.
Marmara varicocelectomy is performed by local or spinal cord anesthesia. It is shown for left-sided and right-sided pathology in men who have an active sexual life. Advantages of this method are:
- no need for hospitalization;
- short operating time( no more than 40 minutes);
- rapid full recovery( up to 5 days, ability to effectively conceive - during the first few years);
- low percentage of relapses( about 1%) and complications.
Goldstein Methodology
A sub-braided microsurgical intervention according to the Goldstein method involves the isolation and dressing of veins( cremasteric, testicular) related to the spermatic cord.
Sequence of the operation:
- incision of 1.5-2 cm at the site of parallel arrangement of veins, near the spermatic cord;
- discharge of the vas deferens, arteries of the testicle( with decreasing pulsation, spraying of papaverine hydrochloride in the form of a 2% solution);
- ligation of large venous vessels with surgical threads( polypropylene d & lt; 5/0);
- suturing the sheath of the spermatic cord;
- vein ligation in the ligament of the lower ovar pole and the membrane;
- layer stitching.
To accurately identify the required vessels, surgeons use head magnification optics or operating microscopes.
Rehabilitation involves an individual selection of therapeutic and prophylactic measures and a set of physical exercises for rapid recovery. During the postoperative period, the spermiogram results are monitored regularly.
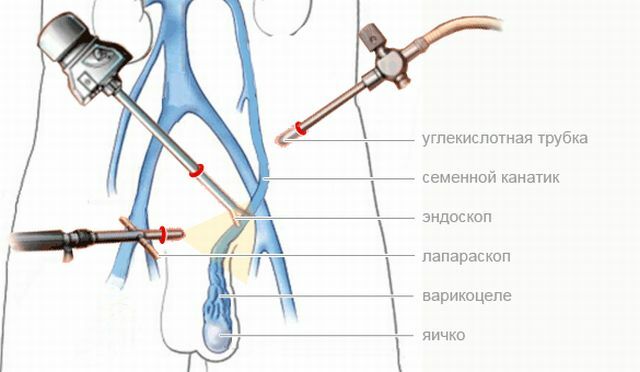
Treatment with laparoscopy
During the operation, a laparoscope is used - a special endoscopic device consisting of a long, flexible tube. At the end is a mini lighting device and a video camera. Everything happening inside is displayed on the monitor.
Laparoscopic operation with varicocele is carried out in this order:
- , laparoscopic ports are inserted through 3 punctures in the anterior wall of the abdominal cavity( 10 mm near the umbilicus - for the video camera, 5 mm in the left anvil, similar to the 5 or 10 mm on the right);
- with the help of a tool isolate the spermatic vein;
- on its branches superimposed titanium staples;
- the area between the main venous vessel and the staple intersects.
The operation is performed under general anesthesia. Its advantages include:
- a full review of the entire length of the seed vein;
- the possibility of simultaneous therapy of pathology on two testicles;
- low probability of relapse( less than 2% of the total number of cases), consequences;
- is a short period of postoperative recovery with fewer restrictions.
The method is indicated for idiopathic form of the disease, in the presence of pain syndrome. Contraindications: the presence of multiple similar surgical interventions in the inguinal, subpowers, acute inflammatory processes in the body, education in the abdominal cavity of various etiologies.
Endovascular surgery
Endovascular occlusion involves intravascular occlusion of the enlarged spermatic vein. There are the following methods.
Sclerotherapy of the seminal veins
The essence of the method is to introduce a sclerosing agent through a catheter passing from the femoral vein into the semen. After this, the walls of the vessel are soldered.
Pros:
- local anesthesia;
- minimum cut - 0,5 cm;
- preliminary phlebography, allowing to examine the lobate venous plexus.
The technique is shown to patients of adolescence, and to adult men in the absence of concomitant diagnoses of the genitourinary system.
Electrocoagulation
Under the action of a low-frequency current, the wall of an enlarged vein adheres. The method has a mechanism similar to sclerotherapy.
Embolization of veins
 A puncture of the femoral, jugular or subclavian vein is followed by the introduction of a 2 mm thick catheter into the renal, then an ovarian venous vessel.
A puncture of the femoral, jugular or subclavian vein is followed by the introduction of a 2 mm thick catheter into the renal, then an ovarian venous vessel.
The lumen of the seed vein is filled: with a special silicone balloon, metallized spiral, occluder, ivanoval seal.
In order to study the state of the veins of the urinary and urogenital system before the operation, they are filled with a contrasting agent( phlebography).If necessary, combine mechanical ablation techniques with sclerotherapy.
Advantages:
- phlebography makes it possible to diagnose concomitant pathologies of venous vessels;
- local anesthesia;
- no scarring;
- low relapse statistics.
After manipulation, the patient should observe bed rest for several hours. Then 2-3 days should limit physical activity.
The effectiveness of conservative and radical treatment of
The fear of postoperative complications causes many people to look for alternative ways to solve the problem. But the only effective method of eliminating pathology is surgical intervention.
Conservative treatment is used as an adjuvant therapy and in idiopathic( primary) form at the time of puberty. In the preparatory and post-operation period, in the presence of intense pain, symptomatic treatment is prescribed.
To stop the attack apply drugs of the group of anesthetics, anti-inflammatory drugs.
Post-operative consequences of
The probability of development of the consequences depends on the chosen method of conducting the operation, the presence of concomitant diagnoses, the patient's age and the stage of neglect of the varicocele. The most common are:
- scrotum lymphostasis;
- azoospermia;
- oligozoospermia;
- hypotrophy, testicular atrophy;
- hydrocele.

Possible consequences of varicocele
Thrombophlebitis of the venous plexus, perforation of the vascular walls is a very rare phenomenon. In order to prevent infertility after the operation, it is necessary to monitor the parameters of the spermogram.
Opinion of patients
Reviews of men who underwent surgery to remove varicocele.
Excruciated pain in the scrotum, turned to the andrologue. Have directed on operation. An experienced doctor performed surgical treatment according to the Marmara method. A week later, I forgot about the former discomfort. Several months passed - no complications. A full sexual life.
Pavel, 40 years old
I did not dare to do the operation for a long time, but I could not stand the pain. Have made a sclerotherapy on the left testicle. There was not even a scar left. After 10 months, I underwent a second examination with contrast. The doctor did not find any violations. I feel good, no drawing pain.
Дмитрий, 16